
The Structural Heart and Valve Center at NYP/Columbia has long been a leader in catheter-based treatment—the least invasive therapy—to repair the mitral valve. This valve regulates blood flow between the upper and the lower chambers on the left side of the heart. When it is damaged or defective, blood flows back up into the upper chamber, producing Mitral Regurgitation (MR).
Patients with MR often have a heart murmur (a turbulent or whooshing sound picked up by a stethoscope) and may suffer from heart palpitations, shortness of breath, fatigue after exertion, and swelling in the feet or ankles. As their valve disease progresses, patients with MR may experience other problems including heart failure, a condition in which the heart can’t pump enough blood to meet the body’s needs.
Because our volume is one of the highest in the country, our Center is one of the first to study and test new devices for heart valve repair and replacement. As a result, our patients benefit from the latest therapies.
The following clinical trials promise to extend our range of options for patients not fit enough to undergo the rigors of conventional surgery. These catheterbased approaches are also referred to as “percutaneous” (meaning “performed through the skin) since no surgical incisions are necessary. Another advantage: The patient doesn’t have to be placed upon a heart-lung machine during these procedures. Because the following treatments are minimally invasive, they are generally associated with a significantly faster recovery time and a lower overall risk.
The COAPT Trial: More Data on the MitraClip
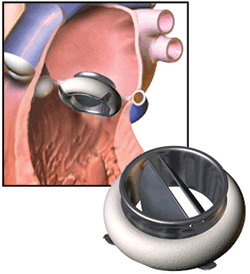
 This major multi-center trial will evaluate the MitraClip, the first catheter-based treatment for patients with MR whose valves leak due to depressed heart function. The MitraClip was patented by physicians at NYP/Columbia. A clip is mounted on the end of a catheter then threaded through a vein in the groin into the right atrium. The clip is opened (its ends parting like the two legs of a clothespin) as it passes through the mitral valve. When the heart contracts, the ends of the clip grab onto the flaps of the valve. The clip is then moved into the “closed” position, pinning the flaps together. The result is a bow-tie-shaped opening that permits blood flow when the heart relaxes, but prevents any leakage or back flow, when the heart contracts.
This major multi-center trial will evaluate the MitraClip, the first catheter-based treatment for patients with MR whose valves leak due to depressed heart function. The MitraClip was patented by physicians at NYP/Columbia. A clip is mounted on the end of a catheter then threaded through a vein in the groin into the right atrium. The clip is opened (its ends parting like the two legs of a clothespin) as it passes through the mitral valve. When the heart contracts, the ends of the clip grab onto the flaps of the valve. The clip is then moved into the “closed” position, pinning the flaps together. The result is a bow-tie-shaped opening that permits blood flow when the heart relaxes, but prevents any leakage or back flow, when the heart contracts.
The COAPT trial will help determine the best way to manage patients with moderate to severe functional MR. If the trial shows benefits with the MitraClip, many more patients may soon be eligible to receive this effective therapy.
The GDS Accucinch: An Adjustable Solution
A second trial will focus on the GDS Accucinch System—another new transcatheter approach to mitral valve repair. This device was designed to reduce congestive heart failure in MR patients who aren’t healthy enough for surgery. Placed through an artery in the patient’s groin, it cinches the mitral annulus—a ring shaped structure that anchors the mitral valve and separates the top and bottom chambers on the left side of the heart. Cinching the mitral annulus helps increase contact between the mitral valve leaflets and stems the backward flow of blood through the mitral valve.
According to the study leader, Dr. Martin Leon, “With the GDS Accucinch System, we can properly size the mitral opening by measuring MR in the beating heart.” These are adjustments that cannot be made while the patient is on a heart-lung machine during traditional open surgery.
The Neochord System: Artificial Muscles Support the Valve
The Neochord System uses artificial muscles to repair this defect. These cords can be applied without the use of a heartlung machine. They are placed on the diseased portion of the mitral valve through a small incision in the chest. A national trial of this device will begin in early 2017, and will be led by Dr. Michael Borger, Director of the Cardiovascular Institute. “The Neochord system has been used in Europe in many hundreds of patients with good results,” says Dr. Borger. “This exciting technology will soon be available in America for patients with a prolapsed or abnormal mitral leaflet and MR.
Advances in Mitral Valve Replacement
 Mitral valve repair has long been considered preferable to replacement because the valve is intimately connected to the functional anatomy of the left ventricle. However, when repair can’t be performed successfully mitral valve replacement is an option.
Mitral valve repair has long been considered preferable to replacement because the valve is intimately connected to the functional anatomy of the left ventricle. However, when repair can’t be performed successfully mitral valve replacement is an option.
The techniques of transcatheter mitral valve replacement (TMVR) are still evolving and we currently have several trials underway to evaluate the safety and feasibility of this approach. These studies will help us answer to the following:
- What forms of valve disease are best treated with TMVR?
- How safe is TMVR?
- How much valve leakage occurs after TMVR?
- After TMVR, is there any recurrence of mitral valve regurgitation over time, and if so, how much?
- Is TMVR equal or superior to surgery? Equal or superior to MitraClip?