By Craig Smith, MD
Article first published on Dr. Smith's Substack, Long Incision.
On May 7, 2026 I had the honor of delivering the keynote address at the ninth annual induction ceremony of the Academy of Clinical Excellence, recognizing sixteen newly elected members. What follows is a lightly edited text of my address.
I will begin by being as precise as possible about what “clinical” means. I surveyed several dictionaries, and prompted Gemini, ChatGPT, and Claude. Britannica wins for brevity: “[Clinical means] work done with real patients.” Combining all sources with my own biases, I’ll embroider that a bit. “Clinical” is indeed patient-centered, but it also aspires to be precise and objective, as in evidence-based. Importantly for our purposes, “clinical” is practical more than theoretical, and practical more than instructional.
Next, why is clinical excellence important? Major academic medical centers have three dimensions—research, teaching, and clinical practice. One time-worn metaphor compares such places to a three-legged stool, but a three-legged stool with uneven legs falls over, and while that aspect of the metaphor makes sense for an institution, it is almost irrelevant to individual faculty.
I prefer to think of our institution as a factory with three floors. I submit that what we call “clinical” is the essential, foundational first floor of every great academic medical center. The research and education floors above can be the same size or smaller, but if that clinical first floor is unproductive, the floors above it wither and die. If we apply my three-floor-factory metaphor to individual faculty, the architecture and interior design is much more flexible. They can put whatever they want on their first floor, and even leave the floors above as dusty shell space. But when we aggregate individuals into our institution, the load-bearing first floor of my factory is sustained by those who are clinically excellent.
Take cardiology as an example, which is the non-surgical specialty I know best. I encourage you to engage in the fanciful experiment of building a great division of cardiology around basic science leadership, and ask whether that division, or any division so conceived, and so dedicated, can long endure. That ground has been hallowed many times—the answer is “no.”
You might be wondering why an Academy of Clinical Excellence (ACE) was established. The goal was to address a longstanding faculty grievance, which goes like this: the best physician-scientists are anointed with the prestige of tenure, but there are no comparable laurels for those clinicians who stand as much above the common lot of doctors as our tenured faculty stand above the common lot of investigators—in other words, no recognition for those clinicians who are “excellent” to the same extent, even if not in exactly the same way, that tenured research faculty are excellent.
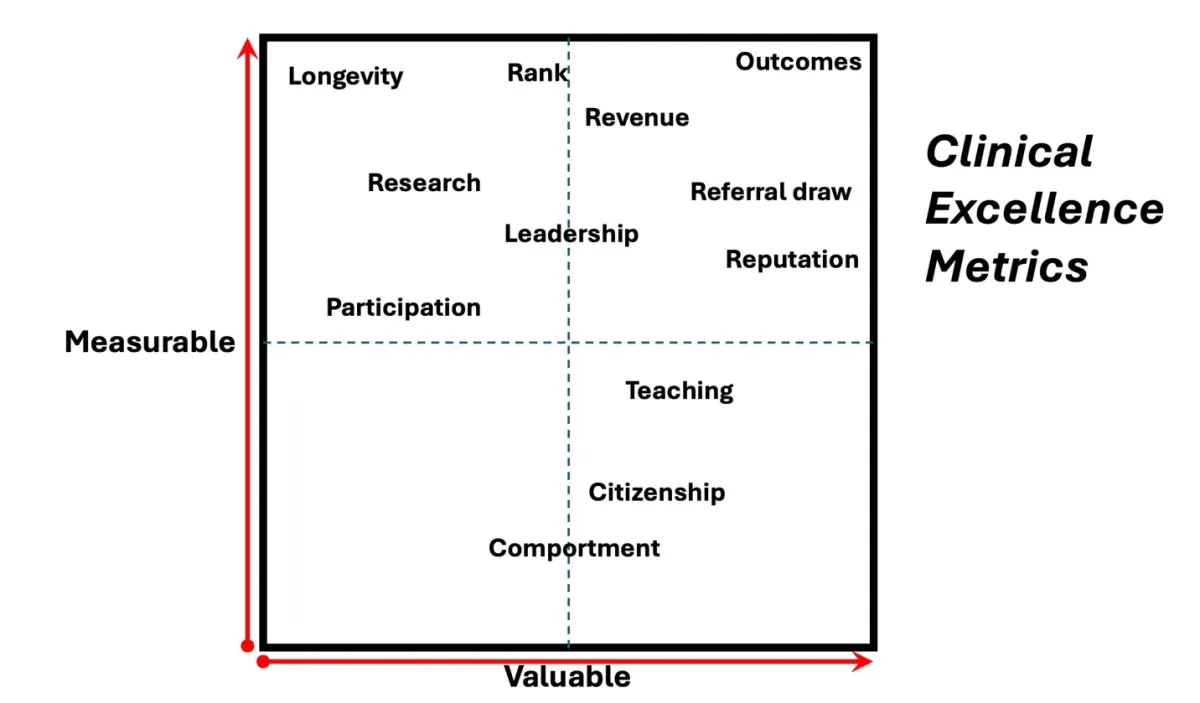
That’s the “why” of singling out clinical excellence, but now comes the hard work of fleshing out the excellence part. This four-quadrant plot is my personal, idiosyncratic attempt to make sense of it. Each of you might do this differently and I encourage you to make up your own.
Let’s sample clockwise around the grid, starting with the left upper quadrant, where things are easy to measure, but not very valuable as metrics of clinical excellence. Longevity and academic rank are the easiest things to measure on my whole grid, and I doubt many of you disagree with where I’ve ranked them. Yet for the inaugural class of our ACE, all Professors with at least 5 years of employment, and at least 50% clinical effort, were offered membership. So just like the other 118 faculty inducted in 2017, I qualified by having enough time-served on my sentence. Why was it done that way? So the Dean’s office could avoid explaining to those not elected by some other set of criteria why they were being denied even this substitute for the prestige of tenure. The problem of developing a better set of criteria was handed off to the new membership.
Had it been up to me, for the first class I would have required each faculty member to submit their personal top-twenty list of the most excellent clinicians. Even without specifying what “excellent” means, I suspect the individual lists would have had a high degree of overlap. Then I would have applied some logical winnowing process to the overlap designed to identify the top twenty, and make them the inaugural class. We would have set a high bar for admission to a small, admired, and exclusive group with room to grow, a club clinicians would want to join.
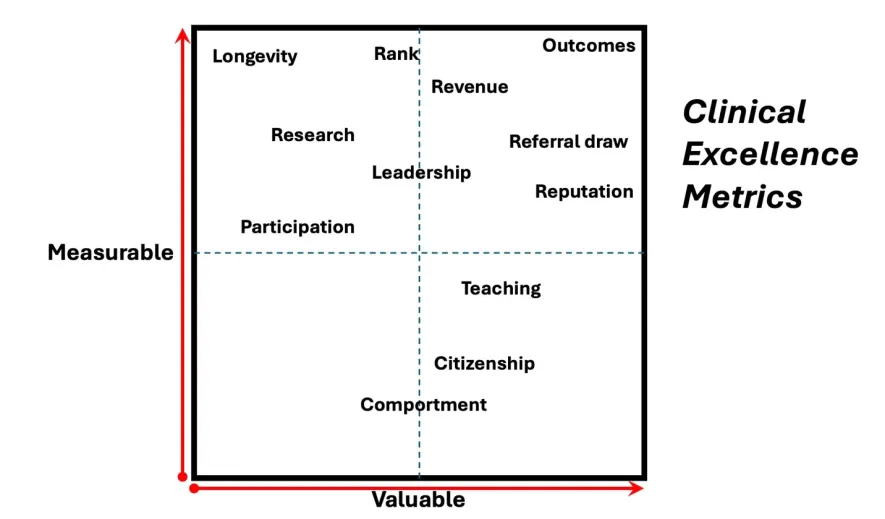
A cohort assembled by the mechanism I just described would lean heavily on attributes that I placed in the right upper quadrant of my grid. I know that not everyone will be excited about the three R’s I’ve placed in that quadrant (Revenue, Reputation, Referral draw). For one thing, they tend to be highly correlated—doctors who draw patients from around the world have towering reputations, and usually bring in lots of revenue, if normalized for their specialty—so am I inflating their importance by expressing them as three things, rather than one? More concerning to many is a belief that the three R’s come with an abundance of individualism, competitiveness, and busy-ness for busy’s sake, traits often considered to be markers of testosterone toxicity and not universally admired in our profession in 2026. If the three R’s rule, instead of A-C-E have we created A-B-N, the Academy of Big Names?
There are other problems with an Academy of Big Names. My right upper quadrant privileges faculty like cardiac surgeons, who are directly other-specialist-facing as well as patient-facing, and who generate large amounts of revenue that appears strongly linked to the individual. The three R’s potentially devalue hospital-based practitioners who might be just as distinguished in their own specialties as any neurosurgeon or cardiologist. Many of us know the standouts in pathology, radiology, or anesthesiology, but few patients or referring specialists have heard of them.
Note what’s sitting in the extreme right upper corner of the right upper quadrant—Outcomes. Being able to show superiority of measurable outcomes is arguably the ultimate marker for excellence, but in most things we do in health care, outcomes are hard to quantify. And where are outcome measures robust? In only a few regulated and closely tracked specialties, like cardiac surgery, that are already highly visible and well represented in my Academy of Big Names. If clinical superstars in many specialties are punished for not being visible enough, even though excellent, our definition of “clinical excellence” needs to offer them a way in. That might require taking a more holistic view of all four quadrants, and maybe metrics should be added that I haven’t thought to include.
Moving on through my quadrants I’ve listed a variety of metrics far softer than outcomes. How much should we value publications, teaching, and roles in leadership or administration? How about things like manners and civility, which I’ve lumped under Comportment? Under Participation, consider the special case in which that means serving on an ACE committee, attending ACE meetings, and educating others in excellence. ACE has decided to emphasize evidence of participation to maintain membership, and considers the probability of active participation in assessing candidates for membership.
This raises a grammatical quibble that I’ve encountered in other organizations dedicated to recognizing professional excellence. Put simply, are we “of” or “for” excellence, in Profession X? “For” captures advocacy for, without quite claiming possession of the virtue itself. In our example, if active promotion of ACE and its goals is an important requirement for membership, shouldn’t we be calling ourselves the Academy for Clinical Excellence? If being the embodiment of clinical excellence is the most basic membership requirement, then “of” is still the right article.
My point is that all the softer metrics I’ve scattered around my grid—like enthusiasm for committee work, teaching, publishing, and comportment—are markers of breadth, depth, and character that embellish clinical excellence. They are wonderful qualities to read about in support letters, and are clearly nice-to-haves, but I’m not sure they’re must-haves.
I’m sure some of you think I’m wallowing in nostalgia, blathering on about what excellence used to be, back in the day. Back when I walked to and from school in the snow uphill both ways. Values change, meaning changes, we change what we call things. “Nostalgia” itself is a great example of that. The term was coined in 1688 by Johannes Hofer, a 19-year-old medical student at the University of Basel, derived from the Greek nostos (homecoming) and algos (pain or grief). He was describing a disease, a pathologic, sometimes fatal homesickness seen in Swiss mercenary soldiers serving at low altitudes. Yet over the past 200 years nostalgia has come to mean an elegiac mixing of idealized history, longing, and regret; kind of a Proustian exercise in performative sentimentality. Meanwhile, the pathologic homesickness Hofer described is now a psychiatric disease called an “Adjustment Disorder with Mixed Anxiety and Depressed Mood,” a kind of “acculturation shock.”
Why this odd detour? Because one thing I’m nostalgic for is the time before national leaders in surgery stood up before a large audience and said things like this: “We must care for the surgeon more than the surgery.” I assume this speaker deliberately avoided saying “more than the patient,” but surgery is how we treat patients. The speaker mentioned in passing sub-arguments like the importance of “extending grace to others and ourselves.” In that, at least the order is right. The airline instruction to put your own mask on first before helping others was mentioned. Certainly true, if seated next to a child. Also invoked was “self-care isn’t selfish”—a semantic platitude that’s not worth dismantling here. But the simple summary is that this surgical leader believes our wellness comes first.
I realize I’m now the patriarchal old white guy peddling his 19th century values to nimbler and less calcified minds. I prefer to think the point I’m making is more timeless and universal. I believe that the most fundamental part of being a professional is subordinating self-interest to the interest of your clients, patients, whoever or whatever. If we should care for the surgeon more than the surgery, should we care for the lawyer more than the law, for the politician more than governing, for the soldier more than victory in battle, for the artist more than art? Dare I even mention caring for the parent more than the child? Do we put me ahead of the mission? Doctors, I urge you, for every minute of every hour of every day when you’re not functioning in your professional capacity, go all-in, 100%, on self-care—that’s what I do!
No doubt you’re wondering what on earth my little sermon has to do with metrics of clinical excellence. Here’s the thing: I’ve read hundreds, even thousands of letters of recommendation—for faculty recruits, resident candidates, med students, college students, etc. But I’ve never read one like this:
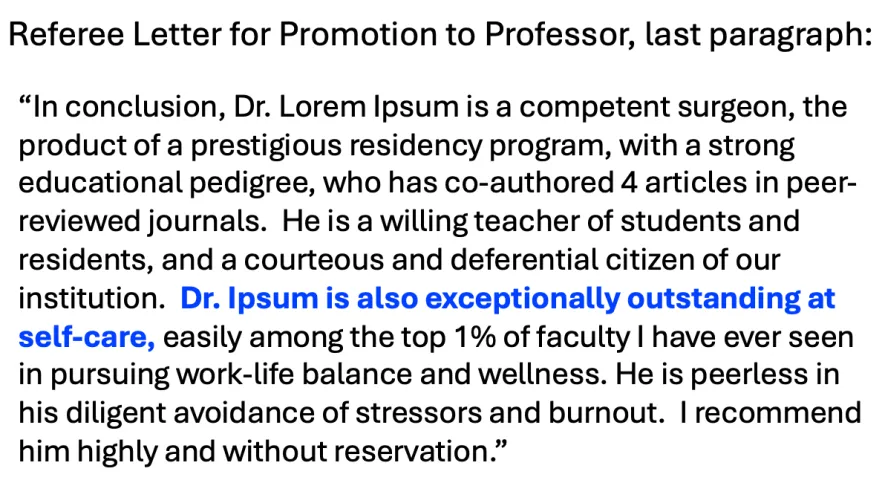
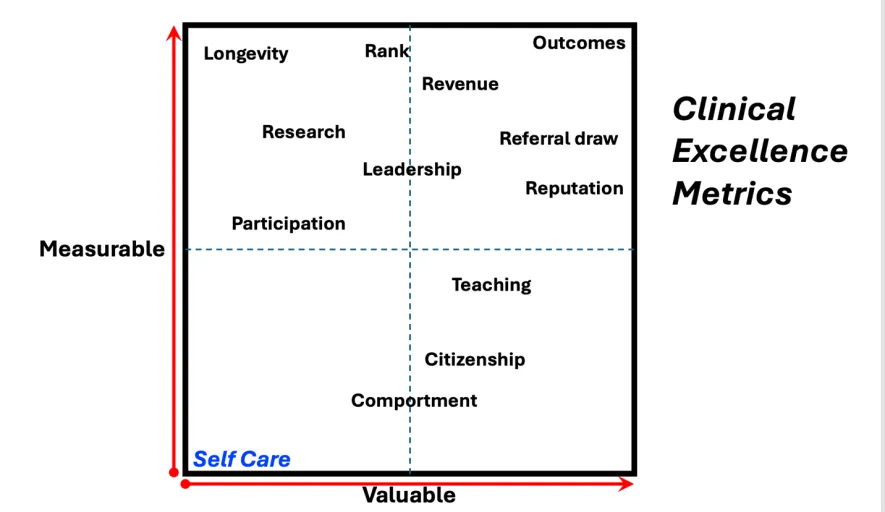
You can probably guess where I would put self-care on my quadrants.
Thank you for allowing me to have some fun getting that off my chest! There are less antagonistic and more compelling reasons not to make wellness a first priority. Consider this simple cartoon I’ve borrowed from DOGHOUSEDIARIES (generously brought to my attention by Dr. Paul Corona, from the Kellogg School of Management at Northwestern University).
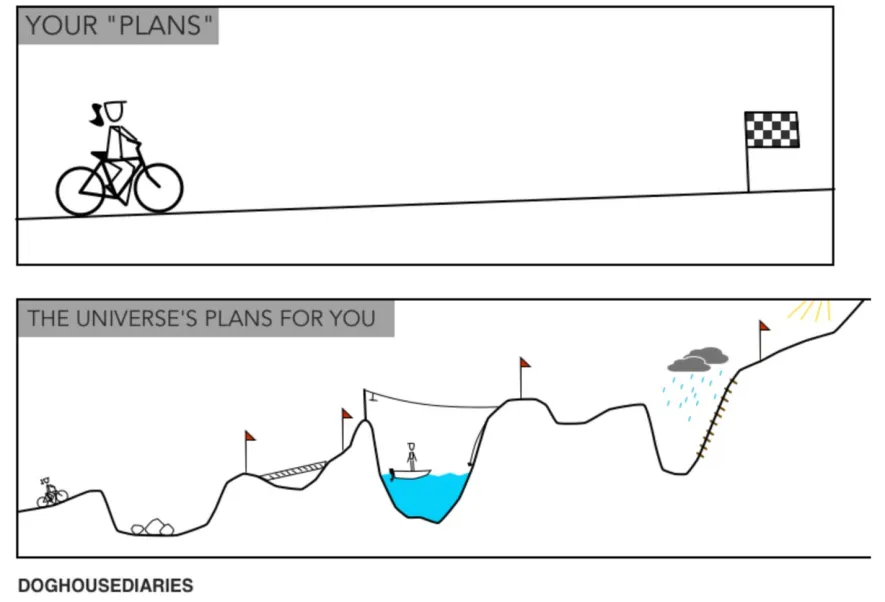
It’s obvious these two journeys are very different. At first glance, the message looks passive and avoidant: “All I want is a smooth, easy ride to the finish, and look what the universe throws at me!” But look more closely at where the two travelers finish. Sure, you can prioritize your journey, and you’ll probably finish somewhere that’s kinda sorta okay. But prioritize your goals, endure the journey, and you might blow the top off the y-axis, up there where the sun shines through—that’s clinical excellence.
Finally, I’m sure we can all agree that the purpose of this event is not to indulge my quirky philosophy. We’re here to celebrate this small, exclusive group of doctors who are being recognized for their outstanding clinical contributions by being inducted into the Academy of Clinical Excellence. Years from now, some of you may be standing up here in my place. I hope you’ll feel comfortable indulging in your own nostalgia about your profession and the years behind you and ahead of you, not in contrast to other generations, but as a continuation of the eternal quest for excellence.
For more opinions and insights from Dr. Smith, follow his Substack newsletter, Long Incision.
Related:
- Book Review with Dr. Craig Smith — The Conscience of Care: Navigating Health in the Culture Wars
- State of the Union: The Stealth Innovations of Modern Surgical Care
- Lessons Learned: Surgeon Craig Smith Reflects on Career in the OR