
By Lindsay Gandolfo
On the morning of a complex aneurysm operation, Virendra Patel, MD, comes in early, blocks off alone time, and sketches.
In complex aortic procedures, reconstruction is rarely, if ever, straight forward. The map of a person’s vasculature is largely unique; its pathways elaborate and far-reaching. And the aorta is at the center, the largest artery, responsible for supplying blood to the entire body.
If enlargement or dilation develops in the aorta—a condition called an aneurysm—the question for most patients is not if surgery will be necessary, but when. Each case presents distinct challenges that require exceptional skill and creativity to solve.
Some people may have extra arteries to the kidneys or a duplicated inferior vena cava—the large vein that carries blood to the heart. Smaller branches of the vasculature may come off extremely close to main branches. In rare cases, arteries that usually come off the back of the aorta instead arise from the front.
When it comes to the repair of complex aneurysms, knowing an individual’s anatomical abnormalities beforehand helps Dr. Patel, chief of Vascular Surgery and Endovascular Interventions at Columbia University, create a surgical blueprint prior to stepping foot in the operating room.
“I’ve found that really having a plan ahead of time is what makes a difference in terms of outcomes, expeditious execution of the operation, and minimizing what we call visceral ischemia time,” says Dr. Patel.
Visceral ischemia time, also called organ ischemia time, is the amount of time blood flow is turned off to intestinal arteries during surgery, which includes branches that feed the liver, kidneys, and abdominal organs. “Getting blood flow back [to the liver and kidneys] and doing things to protect these organs during surgery are very important,” says Dr. Patel. “The longer it takes, the higher the chance for poor outcome.”
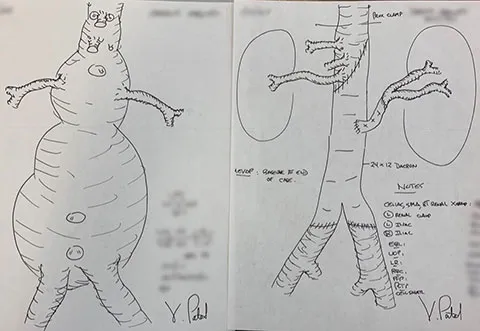
Like his surgical forbearers, Dr. Patel’s planning method involves drawing detailed before and after sketches of the aorta on a piece of paper, an act of preparation born from early study techniques and good ole competitive edge.
“My co-fellow used to do drawings for all of his operations, and I was like ‘what are you doing in the corner over there? And why am I not doing it?’’ Dr. Patel says with a laugh. “So, it started out as ‘Tom’s doing drawings, so I’ve got to do drawings.’”
Soon enough, the artwork paid off in a huge way, “[The attending surgeon] was saying something about how the celiac artery is almost always anterior to the left renal artery,” remembers Dr. Patel. “And I said, in this case, I think it’s on the same level. And he’s like ‘listen I’ve been doing this for 20 years, and it’s never there.’”
But the artery was there, and as soon as his attending uttered the words “I should have listened to you,” Dr. Patel learned it pays to be prepared.
“What started out as being a good fellow and being ready for the attending surgeon to ask you questions and being able to answer those questions have now turned into a mental preparation of what I’m about to face.”
Now, the drawings prepare him for exactly where he will encounter problems, often down to the millimeter.
“I will look at the scan, and I’ll start planning where I think the safe sites are to clamp the aorta without showering debris, where I think the anatomy is going to be tricky, and in terms of sewing things together, what arteries I’m going to reattach versus keep together,” says Dr. Patel. “I do this for all complex aneurysms.”
Dr. Patel will often share these drawings with referring physicians, so that they can better understand what their patients have gone through. He draws less detailed versions for his patients too. He likes to sketch a schematic that shows a clear before and after, highlighting areas of concern, what needs to be fixed and what it will look like afterward. Sometimes the drawings help to explain why he might change an expected course of referred treatment.
“Three weeks ago, I showed a patient the drawing and said I know you were sent to me to be treated with a stent, but you have debris in your aorta, all of these branches are very angulated, you have access vessel problems down here,” says Dr. Patel. “And I don’t think it’s going to be the right answer for you because these are high-risk features. Then I was able to show what reconstruction would look like.”
Creative interpretation works on so many levels, and has the added benefit of putting everyone at ease while working toward optimal outcome. “I think it helps impact recovery, absolutely,” says Dr. Patel. “The faster you do the operation, the better you do your organ protection, the better and faster the recovery.”
Learn more about Vascular Surgery
Sign up for our mailing list for more health news and information from Columbia.