By Lindsay Gandolfo
Dedicating one’s life to the management of difficult, complex, or even “untreatable” diseases demands a special kind of hope and resolve. Treating them in children is work unto itself—an unwavering commitment of heart and spirit, 24/7.
Congenital diaphragmatic hernia (CDH) was once regarded as one of these untreatable conditions: a birth defect characterized by the diaphragm’s failure to close properly, leaving an opening that leads to a cascade of severe complications. Through this hole, organs like the intestines, liver, or stomach can migrate into the chest, disrupting lung development and causing them to function erratically—most often with life-threatening consequences. Upon birth, affected newborns struggle to breathe, exhibit rapid heart rates, and display cyanosis, a persistent blue discoloration of the skin indicating insufficient oxygen.

“When I was a pediatric surgery fellow in Washington [DC] from ‘80 to ‘82, I was probably involved with about 25 newborns with this diagnosis,” said Charles J. Stolar, MD, former surgeon-in-chief and chief of pediatric surgery at Columbia/New York-Presbyterian Morgan Stanley Children’s Hospital and now the Rudolph N. Schullinger Emeritus Professor of the Surgery of Pediatrics. “They all died, 100 percent mortality.”
The American Pediatric Surgical Association (APSA) recently honored Dr. Stolar with the Robert E. Gross Award for Excellence in Pediatric Research and Achievement for his work with CDH. APSA’s highest honor has been awarded only a handful of times in the organization’s history to pediatric surgeons whose lifetime commitment and seminal contributions have significantly changed the standard of pediatric care.
Such recognition prompts a profound question: how did a condition once marked by 100 percent mortality undergo such a remarkable transformation over the past several decades?
Breakthrough in Ventilation Techniques
This method relied on pushing high pressure and high volume through ventilators, a technique originally developed for critically ill adults. However, the extreme pressures and volumes often inflicted severe damage on the fragile, developing lungs of newborns, resulting in a low survival rate for babies with CDH.
“We all have a certain amount of carbon dioxide and oxygen in our system. What we learned was that if you use the ventilator at very high pressures and high volumes to blow off the carbon dioxide, the blood vessels will relax. You could push more blood through the lungs,” said Jay Wilson, MD, Senior Associate of Surgery and Critical Care at Boston Children’s Hospital and associate professor at Harvard Medical School, reflecting on his own experiences as a pioneer of CDH treatment in the 80s. “It was state of the art and still led to 80 percent dead kids…We didn't have anything else. There were no drugs; there were no special ventilators.”
Meanwhile, in New York City, Dr. Stolar, along with his surgical fellow Peter Dillon, MD (now Chairman of Surgery at Penn State), and neonatologist Jen Wung, MD, were exploring a radically different approach. “In the laboratory, we were trying to support these newborns safely, and we were using newborn lambs as our model,” explained Dr. Stolar.
Their method revolved around extracorporeal membrane oxygenation (ECMO), an adaptation of the heart-lung bypass machine. ECMO works by draining blood from the body, circulating it through an artificial lung for oxygenation, and then returning the oxygen-rich blood, effectively supporting the patient’s circulatory system when their heart or lungs cannot do so on their own.
Historically, ECMO use in surgery—whether for adults or children—was limited to just a few hours because the direct contact between blood and gas during oxygenation could cause significant damage to blood cells. Efforts to use ECMO over extended periods, like during the 1970 influenza epidemic, were abandoned due to high mortality rates.
“There's only a certain amount of time you keep a patient on one of these artificial lungs,” said Dr. Stolar. “What made a huge difference was the work being done by Ted Kolobow at NIH.”
Theodor Kolobow, MD, a giant in the field of acute lung injury, contributed significantly through his work at the National Institute of Health's National Heart, Lung, and Blood Institute (NIH NHLBI). “He was developing artificial organs, and they created these lung silicone sheets that were thin enough so that the blood and the gas didn't come into direct contact but allowed excellent gas exchange,” explained Dr. Stolar. “Because it wasn't damaging the blood cells, you could do this for an extended period. That was critical.”
“Then we had to learn how to do it safely,” Dr. Stolar added. “Anytime you put blood in an artificial device, it'll clot. We learned how to keep the blood from clotting and how to support nutrition, renal function, and multi-organ support.” This achievement is a rare, if ever, occurrence in medicine: a revolutionary strategy developed specifically for newborns before it was feasible in adults.

The First Case
New York-Presbyterian Morgan Stanley Children’s Hospital, then called Babies Hospital, became the referral center for Diaphragmatic Hernia in the Tri-State Area. One day, a physician in Stanford, Connecticut, called about a baby with CDH in dire need of support. “In those days, the standard of care was to operate immediately and then keep your fingers crossed,” said Dr. Stolar. “We did that, and he was doing okay for a few hours, and then he was dying. And I remember the father and mother wanted to donate his organs for transplant. He was about a three-and-a-half, four-kilo newborn.”
Options were negligible; no development or device from the lab had yet been approved for human use. “I said, ‘We've been doing this work with newborn lambs. We're encouraged, and this would not be totally off the books but off-label. It has not been through our institutional review board yet. This is a totally investigational treatment, but I think your son would be an excellent candidate, and frankly, nothing to lose because he's going to die otherwise,” he explained.
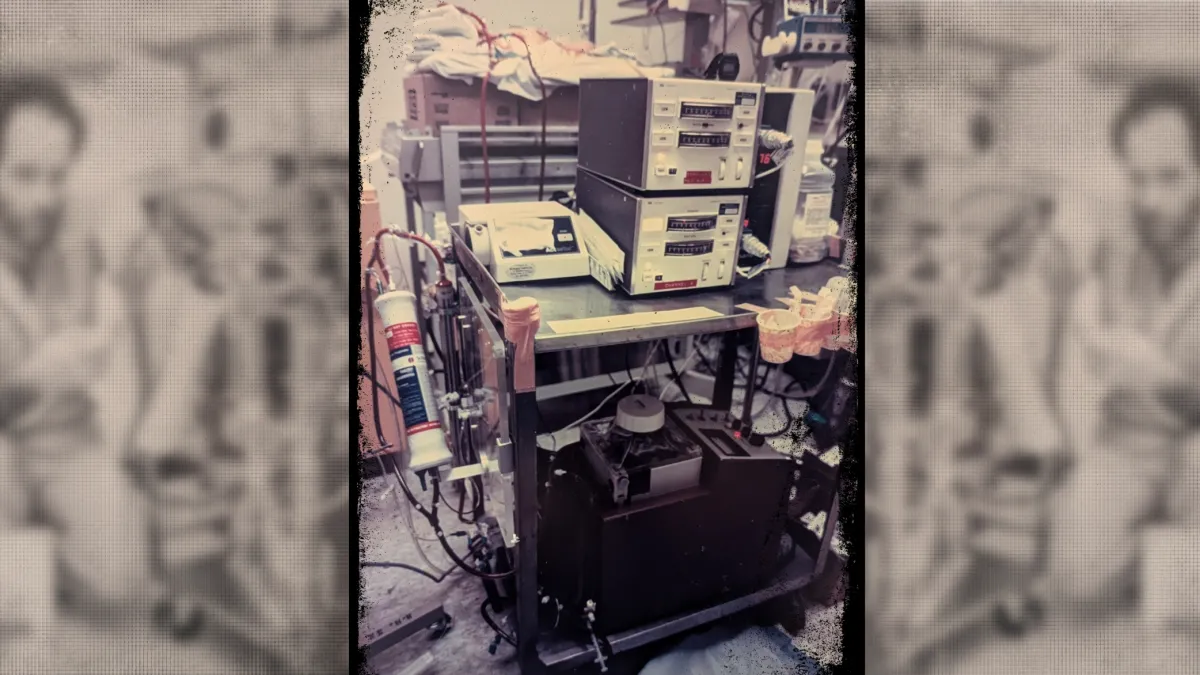
The child’s parents agreed, and Dr. Stolar quickly ushered a stack of makeshift equipment out of the lab and into the clinical realm. “It was a broken-down cafeteria cart with stuff that had been discarded from the cardiac ICU,” he remarks. “Totally MacGyvered and duct-taped together with devices clearly labeled, ‘Not for human use. For animal experimentation only.’”
Beyond parental consent, it should be noted that nothing would have been possible without the support and approval of the then-chief of Neonatology, John Driscoll, MD, and his mentor, L. Stanley James, MD, a coworker of Virginia Apgar, MD (developer of the Apgar Score used to assess newborn health), and founder of neonatology at Babies Hospital. Dr. Driscoll had confidence and said, “Yes, we can do this.”
They commandeered a small room in the back of the neonatal ICU and sprang into action. “We closed the door, and Peter Dillon and I spent 12-hour shifts living there in the NICU with this baby on these artificial organs,” said Dr. Stolar. “We never left this kid's bedside because, quite frankly, we were terrified. This had never been done.” Their round-the-clock, live-in support continued through the week. “My wife Carol and Peter’s wife Judy would bring us meals because we were sleeping in the neonatal ICU every night.”
Then, on the seventh day, as if defying the odds right before their eyes, he started to show signs of improvement. Slowly but surely, that newborn fought his way back. Dr. Stolar and Dr. Dillon soon began the process of weaning him off the devices and extubating him. Today, that same child is a 41-year-old man, married and a father of two.
“That was case number one. Then we became known in the New York area because this kid lived,” said Dr. Stolar. “I'd never seen this diagnosis living, discharged, to turn into an obnoxious teenager. I’d never seen that before.”
Cases of newborns with diaphragmatic hernia began to accumulate more and more, as well as other diagnoses of respiratory failure that had a 95 percent chance of mortality. “Right away, we were converting that [95 percent] mortality to 85 percent survival, a full transformation,” explained Dr. Stolar. “We did not invent it, but we perfected it at Columbia. And we were the first to report dramatic improvement in CDH survival.”
Transforming the Standard of Care
“He and Jen Wung were the only ones pushing this ventilation strategy, and it was voodoo magic to the rest of us,” said Dr. Wilson. “Half the time, we didn't believe their numbers. We just thought they were lying. And no one thought it was a process that could be exported.”
One of Dr. Wilson's first lectures at a national meeting was about CDH and high-pressure ventilation. “That was the first time I met Charlie. He stood up and shredded me, ‘You’re killing babies, you’re killing babies because the ventilators are just too powerful,’” said Dr. Wilson. “And I was really pissed because he made me look bad, and I gave him a pretty blistering answer back. But he really got me thinking, and that was the start of our friendship.”
By then, Dr. Stolar’s data showed babies with CDH do not require excessively high oxygen at high pressure and volume. A new strategy of permissive hypercapnia (or spontaneous ventilation) allowed for ventilation adjustment, using high partial pressure of carbon dioxide to avoid induced lung injury. The combination of spontaneous ventilation with prolonged ECMO support marked a radical shift in the survival of newborns with CDH. In fact, allowing elevated carbon dioxide retention while monitoring oxygen levels closely could, in many cases, prevent the need for ECMO altogether.
“Fast forward a year or so, I’m about to put another kid on ECMO, and I called Charlie up. I said, ‘Alright, you son of a bitch, here’s what I got for numbers; put your money where your mouth is and tell me what to do,” he said.
Dr. Stolar instructed Dr. Wilson on the exact metrics of the ventilator and how low the oxygen could safely go. “I sat at the bedside and called him every 40 minutes all night long. And the kid never went on ECMO. He lived.”
They repeated this intense, all-night process for Dr. Wilson’s next CDH case a week later and then again for a third. “That’s when I learned they were right,” said Dr. Wilson. “So, I totally switched over. The numbers were dramatic and incredible, from 80 percent mortality to 20 percent by the time I finished. Not because I did anything other than prove that he wasn't a liar; it was exportable, and it works.”
In five short years, the practice of spontaneous ventilation was embraced worldwide.

The Ever-Evolving Journey of Improvement
“A lot's happened since then and in the early 80s,” said Dr. Stolar. “We began to realize that this condition wasn't necessarily a surgical emergency but a physiologic emergency. And we learned that it was safe to wait for the baby to get over being born.”
Ordinarily, babies are born with a blue-ish tint and start to turn pink in a matter of seconds, but for babies with a diaphragmatic hernia, this process takes much longer—often several days—due to impaired lung development caused by the hernia. “Their lungs are very nervous. They're jittery and anxious. We learned that instead of stressing the baby out with a big operation right at birth, in the majority of these babies, we could give them some time to calm down,” said Dr. Stolar. “Then we'd do an operation electively instead of in the middle of the night, several days later when it was a very calm, non-emergent situation.”
By delaying treatment, they could better assess the severity of each case, identifying which babies were stable enough to wait and which required immediate ECMO intervention. “The number of infants who needed ECMO became much smaller. The number of diaphragmatic hernias became much more selected in a much sicker, much more unstable population,” said Dr. Stolar. “Delaying the surgery until it's elective, a lot of that work came from Columbia.”
Interventions only grew more and more refined. Nitric oxide and drugs to relax blood vessels were introduced, aiding blood flow and supporting the function of the right side of the heart, which is responsible for pumping blood to the lungs. “That brought another breakthrough,” said Dr. Wilson. “We always thought the kids died of lung disease. Then I started doing echocardiograms on kids, sometimes two, three, four times a day. And I realized that every time the kid went bad, it had nothing to do with the lungs. The right heart was packing it in, and you had to do something.”
Treatment for CDH instantly went from a process of lung management to a right heart failure model of management. “I had a slide that I showed at my next talk, which changed everything,” said Dr. Wilson. “It said ‘congenital diaphragmatic hernia’ and underneath, ‘It's the heart, stupid.’”
Each advancement refined the treatment approach, narrowing down the cohort of infants with diaphragmatic hernias who truly needed ECMO, leaving only the most critically ill and fragile. “The goal was to put ourselves out of business,” said Dr. Stolar. “Because putting a kid on a heart-lung machine for a couple of weeks is not without its hazard. What's happened now is that ECMO survival is closer to 50 percent. Why? Because these other strategies have removed babies that don't really need ECMO. These are a small group, the most challenging. These are the numbers of success.”
CDH treatment protocols also led to the development of an entirely new mode of neonatal ventilation. Other neonatal diagnoses that once would have required ECMO, like meconium aspiration and sepsis, no longer call for it. “We’ve been so successful with these ventilator strategies that don't destroy the lungs and extubate early that the number of newborns who need ECMO are mostly kids with congenital heart defects. Now that’s the most common indication,” said Dr. Stolar.
Thoughtfulness Expands ECMO into New Frontiers
But in this ever-evolving field, progress remains relentless. Fetal surgery is gaining steam. “Now, they can laparoscopically put a balloon that essentially allows the lungs to develop and make it more likely that the kid will make it to term, which wasn’t happening with attempts at open fetal surgery,” said Dr. Wilson. “Right now, standard management still has a higher survival than fetal intervention. It’s not there yet, but they're close. It’s got legs.”
Putting themselves out of business is no hyperbole. Although Dr. Stolar and Dr. Wilson are surgeons, their work vividly illustrates that not every problem labeled "surgical" demands a surgical solution. “I still think we have a surgical solution to a medical problem,” said Dr. Wilson. “There has to be a biochemical answer, a growth factor we can give to grow these lungs.”
The quest to improve survival rates for the most critically ill babies with CDH, even those facing a 50 percent survival rate with ECMO, remains a driving force. “It’s a lot harder than doing an operation, but just imagine the impact of a medical solution, the impact on that infant and now mother,” said Dr. Stolar. “Being thoughtful is hard, but that’s the responsibility we signed up for.”
The sheer impact of this thoughtful approach has expanded far beyond neonatal care. The advancements and applications of ECMO technology that revolutionized care for infants have also transformed the treatment of severe respiratory and cardiac conditions in adults. Today, ECMO remains a cornerstone at Columbia, where groundbreaking work continues to propel the field forward.
Modern ECMO is a far cry from its early iterations. "The early technology used to be that the blood was driven by a roller pump. You had to stop and adjust the tubing every now and then because it would get worn from the roller pumps going around it. The tubing might rupture, or cannulas got dislodged, and it's this spectacular bloodbath in the ICU of really failing in a very dramatic way," said William Middlesworth, MD, pediatric surgeon and Director of the Pediatric ECMO Program at Columbia.
Today’s ECMO machines utilize advanced centrifugal pumps and membrane oxygenators, providing safer and more reliable support. “Now we have pumps that effectively work like a boat propeller suspended in a magnetic field,” explained Dr. Middlesworth. “It doesn't generate heat as it spins, and we think it also has less mechanical wear on the red blood cells themselves.”
One of the most revolutionary advancements in ECMO technology is its portability. "The one we currently use for adults is about 22 pounds," said Cara Agerstrand, MD, Director of the Medical ECMO Program at Columbia. This increased mobility has enabled the creation of fully portable ECMO units, allowing teams to stabilize patients on-site before transferring them to specialized centers, a practice already in use in places like Paris.
ECMO’s evolution represents a major full-circle moment. The institution where ECMO technology initially transformed care for the sickest infants is now once again leading the charge with new, lifesaving applications. “We really tried to expand the knowledge of this technology to the regional area in New York City and New Jersey so other hospitals knew that if you have a really sick patient who might be appropriate for this, give us a call, and we can not only do ECMO, but we can actually come to your hospital, start ECMO there, and then transport that patient back to Columbia,” explained Dr. Agerstrand.
No event in the modern era underscored the vital role of ECMO in managing severe respiratory failure like the COVID-19 pandemic. ECMO use surged and further validated its efficacy in supporting critically ill patients. "As the technology continually improves, I'm sure we'll see a broader expansion and integration into standard ICU algorithms for respiratory failure," said Dr. Agerstrand. “We were able to do it quite successfully and quite safely. And that was a little bit of a surprise to many people who thought, ‘Oh my gosh, it has to be limited to these very select centers.’”
ECMO has also become indispensable in organ transplantation, frequently used as a bridge to lung transplantation for patients who otherwise would not survive long enough to receive a donor organ. “Being able to set up ways that we can have patients exercise and walk while they're on ECMO so we preserve their overall health as much as we can in anticipation of lung transplant is transformative,” explained Dr. Middlesworth. “It improves their outcomes post-transplant.”
“I've been at Columbia since 2006. I do ECMO all the time; that's my specialty. But such a rich historical legacy of innovation stemming back to Charlie's time, its early adaptation and adoption, is a really interesting and special thing to be a part of,” added Dr. Agerstrand. “It’s a unique element of our program. One that has pushed limits and set standards worldwide.”
The unwavering dedication of Dr. Stolar, mirrored by Dr. Wilson and every colleague thereafter, resonates in each life saved by ECMO—an enduring testament to the power of persistence, courage, and innovation. May their efforts, undying spirits, and tireless pursuit of better outcomes serve as an exhortation to all who champion progress in medicine.
Related:
- Tiny Patients, Big Solutions: A Closer Look at Fetal Surgery Innovations
- State of the Union: Lung Transplant Today
- NewYork-Presbyterian Morgan Stanley Children’s Hospital Recognized for Providing the Region’s Best Care