From NYP Advances, a resource for medical professionals by NewYork-Presbyterian.
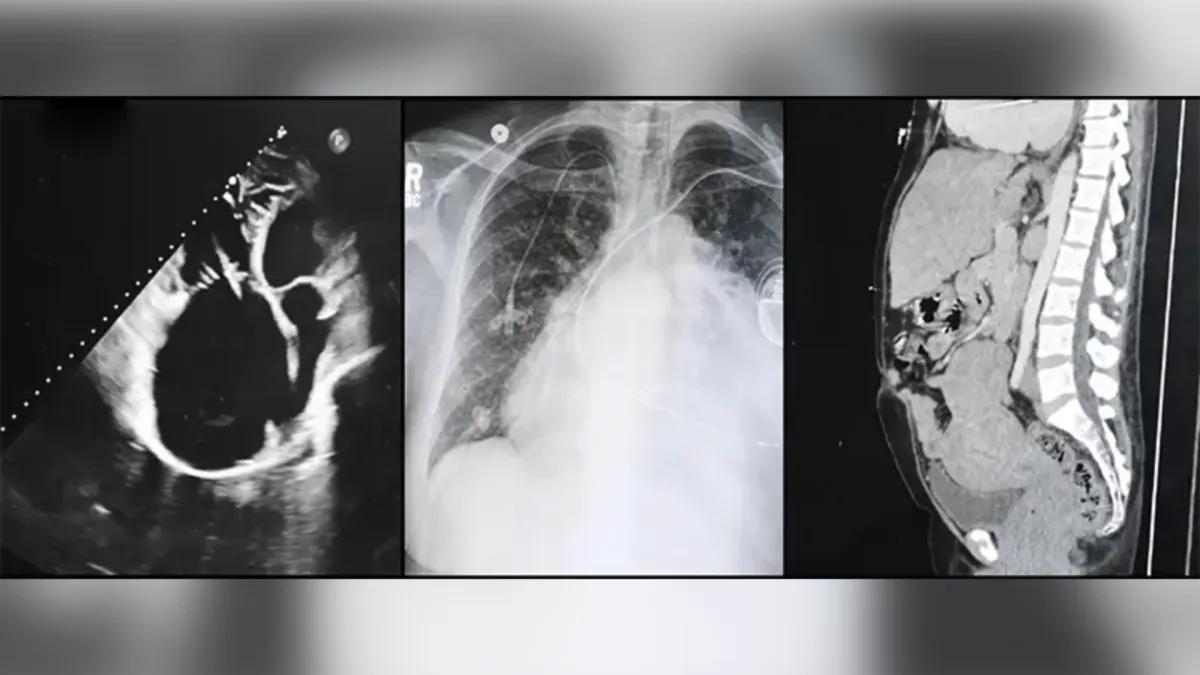
A NewYork-Presbyterian and Columbia transplant team hit a rare milestone last year when they performed a multiorgan transplant on a 50-year-old female patient with pulmonary arterial hypertension, heart failure, and congestive liver cirrhosis: It marked the first time that a heart-lung-liver transplant had been performed in New York.
The 14-hour procedure was the culmination of years of care and months of surgical preparation by a multidisciplinary team that came together to treat a patient with a complex medical history. The physicians who led the patient’s care at NewYork-Presbyterian and Columbia included:
- Tomoaki Kato, MD, clinical director of transplant services at NewYork-Presbyterian and Columbia and chief of the Division of Abdominal Organ Transplant and Hepatobiliary Surgery, who performed the liver transplant;
- Philippe Lemaitre, MD, PhD, surgical director of the Lung Transplant Program, who performed the lung transplant;
- Koji Takeda, MD, PhD, surgical director of heart transplantation and mechanical support, surgical director of the Adult Extracorporeal Membrane Oxygenation Program and director of the Pulmonary Thromboendarterectomy Program, who performed the heart transplant;
- Jennifer Haythe, MD, director of the Adult Pulmonary Hypertension Program and the patient’s cardiologist;
- Selim Arcasoy, MD, MPH, medical director of the Lung Transplant Program and the patient’s transplant pulmonologist; and
- Alyson Fox, MD, medical director of the Adult Liver Transplant Program and the patient’s transplant hepatologist.
While multiorgan transplants have been on the rise in the U.S. in recent years, only 13 other heart-lung-liver transplants have ever been performed in the U.S. as of June 2025, according to the Organ Procurement and Transplantation Network, with NewYork-Presbyterian’s most recent case the first recorded not only in New York but also the Northeast. What makes a heart-lung-liver transplant so rare is that it requires a confluence of factors: a clinical team with the requisite surgical and medical experience; a patient at the appropriate stage of disease progression; and the availability of the organs from a single donor to reduce the risk of rejection.
“As a high-volume center, NewYork-Presbyterian has done different combinations of multiorgan transplants, giving us the unmatched skill, experience, team collaboration, and surgical and medical integration to do this heart-lung-liver transplant,” says Dr. Kato. “From the beginning to the end, altogether it went flawlessly, and our teamwork resulted in this great success.”
The Road to a Triple Transplant
The patient, Nadine Davis, came under the care of Dr. Haythe in 2012. She had been diagnosed with pulmonary arterial hypertension (PAH) several years earlier, but her condition was slowly getting worse. She remained on three oral medications aimed at lowering pressure and dilating the blood vessels in the lungs until about 2014, when the care team decided to advance treatment and add a continuous intravenous infusion with an indwelling catheter.
Several complications arose: Nadine developed an IV line infection, leading to endocarditis, which was treated with antibiotics. However, the infection left her with a leaky tricuspid valve, but she could not undergo tricuspid valve replacement because her PAH made general anesthesia life-threatening. Separately, surgeons implanted a pacemaker to address a heart block, a heart rhythm disorder that disrupts how the heart beats.
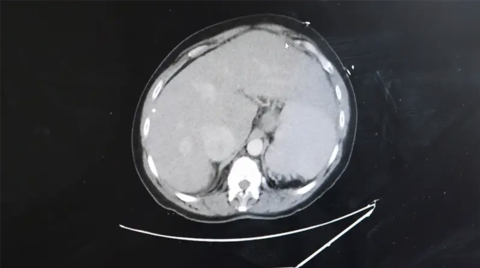
By 2023, Nadine had developed right heart failure, which caused congestion in her liver and led to liver cirrhosis. The natural progression of pulmonary arterial hypertension usually results in lung transplantation, according to Dr. Haythe, so she referred her to Dr. Arcasoy for lung transplant evaluation. The team listed her for transplant in January 2024.
“After evaluation, the best option seemed to be a combined heart-double lung-liver transplant due to poor organ function,” says Dr. Arcasoy. “Early referral was key in this case, because if it had been later in the course of her pulmonary hypertension, there would have been no way of us getting her over the finish line to be listed and transplanted in a healthy-enough state.”
In March 2024, Nadine was admitted to the ICU for pneumonia, where she stayed until the end of April while on the transplant waitlist. It was then that the clinical team received the call: there was a pair of lungs, a heart, and a liver, all from the same deceased donor, available.
“In order for a transplant like this to come together, everything had to align. If the patient is too well, you can’t send them for transplant. If they’re too sick, they can’t undergo the surgery,” says Dr. Haythe. “This was the right moment — and when you’re able to follow a patient as closely as we can, we can detect when those moments happen.”
Mapping Out the Surgical Strategy
Although the call came in April, the preparation for transplant had started months prior. The teams had conducted huddles to organize personalized surgical and post-transplant protocols for Nadine.
“Figuring out how we are going into the surgery is just as important as the surgery itself: hashing out the details and sequencing, from when we receive the organ call to the selection to the order of the procedures — everything had to be perfect,” says Dr. Kato.
By the time the donor call arrived and the organs were reviewed and accepted by each transplant team, they were well prepared. On April 30, 2024, the triple transplant began with the heart and lungs en bloc — meaning the organs are implanted together — with Dr. Takeda and Dr. Lemaitre working in tandem in the operating room.
After Dr. Lemaitre opened the chest with a clamshell incision through the breastbone, Dr. Takeda placed Nadine on cardiopulmonary bypass to remove the heart; then Dr. Lemaitre took over to remove the lungs.
“We remove each lung, taking great care to not injure the phrenic nerves that innervate the diaphragm,” says Dr. Lemaitre. “For lung transplantation and heart-lung transplantation, it's nearly the most important structure we want to preserve because if the diaphragm doesn't work, the patient cannot breathe after the operation, which defeats the whole purpose.”
Once the tracheal anastomosis was completed, Dr. Takeda connected the superior and inferior vena cava and performed aortic anastomosis to complete implantation of the thoracic organs. Dr. Kato and the liver team then entered the operating room to perform the liver transplant.
After the liver was in and the abdomen closed, Dr. Lemaitre took over again to determine whether to close the chest. “We decided to leave her on respiratory support with an ECMO device that basically allowed the lungs to recover gently, and we left the chest open for 48 hours before closing,” he says.
Coordinated Care in Recovery
For post-transplant recovery, the ICU and heart, lung, and liver transplant teams rounded together in the mornings to discuss care coordination and visit Nadine, and at the end of the day checked in remotely to adjust medications based on her lab results and progression.
Nadine was discharged two months post-operatively. She receives follow-up care every six to eight weeks that is managed by the lung team, and visits with the heart and liver teams to undergo bronchoscopies, echocardiograms, blood work, and biopsies.

The lung team treated two bouts of rejection with corticosteroid pulses and maintenance immunosuppressive therapy, and Nadine continues cardiopulmonary rehabilitation for functional muscle strength.
“To be able to help a person who is very sick with limited lifespan and get her to a much better functional state with good quality of life, extended survival, and happiness, is the ultimate gift that we could get,” says Dr. Arcasoy, who follows Nadine post-transplant.
“What makes NewYork-Presbyterian special is that you can’t have a successful triple transplant unless you have excellence in so many different areas. From nursing and pharmacy to social work and psychiatry, this is a massive team effort,” adds Dr. Haythe. “This is a very high-level, complicated execution. It’s like an orchestra, and when it works, it’s beautiful.”
Related:
- State of the Union: Lung and Chest Care Today
- A Look Inside the 24-hour Dance of a Split-Domino Heart Transplant
- Changing the Future of Living Liver Donation: A Conversation about Columbia’s All-Robotic Approach