
Reviewed January 2022 to maintain the latest information in treatment and research.
An interview with Hiroo Takayama, MD, PhD, Co-Director of the Aortic Center.
Before we get into the latest updates in aortic care, will you walk us through the complex anatomy of the aorta?
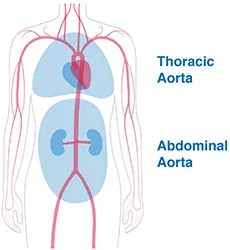
The aorta is a blood pipe, an artery, that’s the largest vessel in the body. It starts from the heart and goes all the way to the legs. On the way, it branches out to provide blood flow to a variety of organs, including the brain, liver, intestines, kidneys, then arms, legs, et cetera.
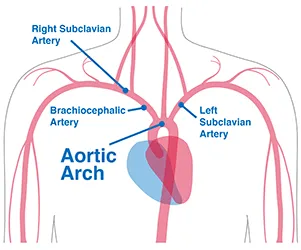
Specifically, the beginning of the aorta takes off from the heart with the aortic valve situated between the aorta and the heart. Next is your aortic root, the bottom part the aorta connected to the heart. This is where the aortic valve meets the branch of the coronary arteries [the arteries that feed the heart]. Beyond that point, the blood first flows upward towards your head in the ascending aorta. Then, the aorta makes a 180 degree turn downwards towards your back. Where the aorta makes that turn is called the transfer aorta or aortic arch. From there, branches extend to provide blood to the brain and the arms. The next long section after the turn of the arch is the descending aorta, sending blood downwards along the spine, leading right into the diaphragm (the membrane that separates the abdomen from the chest). The abdominal aorta continues downwards beyond the diaphragm until it bifurcates right and left toward the legs. And that is the end of aorta.
That was a supremely helpful explanation. Let’s jump in, what’s new in aortic care?
You know, aortic surgery, especially thoracic aortic surgery, is usually done to treat aortic aneurysms or complications related to aortic aneurysms—like aortic dissections, or aortic rupture. What's significant about those aortic complications, or aortic aneurysm, is that once you develop complications the majority of those patients die within 24 hours.
What is an aortic dissection exactly?
Aortic dissection is when the lumen [the normal passageway for blood] in the aorta gets split into two. So, all of a sudden, you develop a flap in the middle of the blood pipe. And the aortic wall is composed of several layers, so, say you have a tear in the most inner layer of the aortic wall, called the intima. When there is an injury in the intima, blood sneaks in between the layers of the aortic wall. That elevates the intima toward the middle, towards the lumen, and becomes a flap. Creating aortic dissection.
That plane extends distally, all the way to the legs, or proximally, all the way to the heart. And by the way, if an intima injury occurs all the way through, that's an aortic rupture. Imagine this now, if you develop an aortic rupture you just die there. Suddenly. The goal of treating aortic disease is to do surgery before those complications happen or when the complications happen. And recently we have had such advances in therapies, especially with the use of transcatheter or endovascular therapy, in combination with open surgery, that we can do so much more.
When would you use open surgery as opposed to minimally invasive treatments?
Open surgery is applied in the more proximal end of the aorta. If your artery dissection is closer to the heart, with the current technology, we still cannot apply this endovascular therapy. Although, we do it when the anatomy and the conditions are perfect. Nonetheless, open surgery remains the gold standard. And for that, we have been developing a variety of new surgical techniques that allow our patients to preserve their own valve, which is huge. There has been so much progress in this area in recent years.
Can you explain the spectrum of aortic disease when talking about dissection and aneurysms? How important is early detection? What does that look like?
The reason why in the beginning I said the majority of the conditions that we treat are aortic aneurysms is because aortic aneurysms are a strong risk factor or precursor condition to developing those catastrophic aortic events. In that sense, it is definitely important to treat it before something bad happens. The difficulty with aortic aneurysms is that unless it's in a specific location or has specific characteristics, it does not cause any symptoms. You may have it, but you don't know it. This is where screening or follow-up becomes important.
Wow.
I’ll give you a common scenario. You go to your primary doctor with a variety of symptoms, say cold or flu-like symptoms. They do some routine work-up, including chest x-ray or EKG. Then they notify you of sudden subtle abnormal findings on the EKG or the x-ray. That triggers you to have an echocardiogram. An echocardiogram may accidentally or incidentally identify a dilation, or enlargement, of the aorta. That's often how patients discover they have an aortic aneurysm. And these patients are usually pretty young and healthy.
Have advancements in imaging helped in this regard? Are you now able to detect more aneurysms with new technology?
That's a very good question. In the past, obviously, we had echocardiogram, we had CT scans, and we had some MRIs and chest x-rays. But currently, we use echocardiograms, CT scans, and MRIs together. And each of them have become very advanced. Particularly, the CT scan and the MRI have made a lot of progress in image quality. The benefit of the MRI is that you don't receive any radiation, but the downside of the MRI, still to some extent, is the spatial resolution. The spatial resolution of the aorta or the cardiovascular structure that an MRI provides is not perfect. Though it is getting better and better over time.
Now, the picture can be synchronized with your heartbeat, and this is particularly important when we talk about the part of the aorta that's close to the heart: the aortic root and the ascending aorta. Since those parts of the aorta are attached to the heart, they move with the heartbeat. Until recently, images around that area were limited or would appear looking like a blob. Measurement was sometimes off, but with this synchronized technique, we can get a much clearer image with MRI.
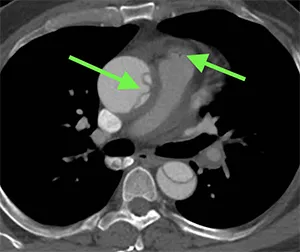
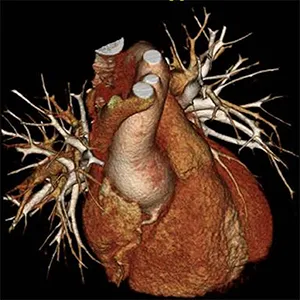
With CT scans, the imaging is actually even more prominent. What we use is called an EKG-gated CT angiogram, which also synchronizes with the heartbeat. And we use them routinely in surgical planning, especially if you are undergoing surgery with a very precise measurement. It provides us with a beautiful image of the heart and of the aorta. We also now have special software that allows us to do 3D reconstruction of the image.
Amazing. So how often do you do MRIs, CTs, and 3D reconstruction in patients?
In every single case, we use these techniques together. And that’s become routine in the past five, six years, especially that kind of detail and anatomical evaluation.
Has this advancement in imaging also helped assist in the new devices and the new types of procedures you can do, whether endovascularlly or minimally invasively?
Absolutely. The imaging is critically important when using the endovascular approach, where you place a graft through a catheter. The graft is a two-layer structure that has a scaffold and sits inside of the blood vessel. The outside of it is covered by a synthetic membrane. So, the graft is placed inside the aortic structure, excluding the aneurysm from the bloodstream. Basically, what happens is the aneurysm shrinks after a placement.
How long can a graft stay in place? Do you ever have to get it replaced at all?
As long as it’s placed the right way, it’s good for the rest of the patient’s life.
And that is where good imaging becomes extremely important. Unlike open surgery, we have to determine the size of the graft or the placement of the graft by looking at the CT scan or the angiogram. The imaging is inspected extremely carefully before the procedure. This allows us to determine whether our patient has what we call “good anatomy” for such a minimally invasive approach.
What constitutes “good anatomy” for minimally invasive surgery?
The concept of endovascular therapy is called TEVAR, Transcatheter Endovascular Aortic Aneurysm Repair, where we place a graft inside of the blood vessel to exclude the aneurysm. To do this we need landing zones, a certain length of healthy aorta to place the device because they sit there without any sutures. You know, in a sense the graft is floating within the aneurysm, it actually uses radial force to place itself against the aortic wall. And there are proximal and distal landing zones, where the aorta has to be within a certain diameter and have good structural integrity. That’s why we use the guidance of the CT scan to precisely understand what these landing zones look like. There is a lot of thought that happens before the patient goes into the operating room. We spend hours examining the CT scan, echocardiogram, and the MRI.
Since the Aortic Center is a collaboration between you, a heart surgeon, and Virendra Patel, MD, a vascular surgeon, is this preparation something that you do together?
Absolutely. V [Dr. Patel] and I share literally every single aortic case. For instance, last night I was operating on a young Marfan patient, we were doing an open surgery aortic arch aneurysm repair and operated together until midnight. That's a very unique feature of this program. Many places say they have a multidisciplinary program, but we really mean it. We’re very, very proud of our tight collaboration. We see our patients together before and after surgery too.
Is that the case even now when using telehealth and virtual visits?
Oh yeah, we both sign in for every appointment.
That’s great. Let's talk more about Marfan syndrome now that you brought it up. Have there been any changes in how that's treated or how other connective tissue disorders are treated?
Yes. You know, these patients are tough. They have a genetic disorder that disrupts the connective tissue. When Marfan syndrome was first discovered, the average life expectancy was around 40 years old. And that landscape has changed dramatically, patients live well into old age now mostly because of the prophylactic [preventative] aortic surgery. Marfan patients and people with Marfan-related syndromes often die of aortic dissection or aortic rupture (like we discussed earlier). By examining these patients carefully over time, we learn when to do a prophylactic surgery, and that transforms the prognosis.
So, in a Marfan patient, we carefully watch the behavior of their aortic root to see if it expands or becomes enlarged, and that’s usually when we do surgery. These patients are young and otherwise healthy, you know, these very athletic people, basketball players. Historically, we used to replace the aortic valve, but that’s far from ideal in young, active patients. They have to be on blood thinners for the rest of their lives.
Now there is an operation called Valve Sparing Aortic Root Replacement, where we don't have to replace a valve. Today, we’re preserving their valve before something bad happens. Imagine if we didn’t do that—they would likely die at the scene of dissection or rupture. And even if we were able to save them with an emergency surgery to replace the aortic root, say in the ascending aorta, in the arch, the descending aorta and beyond would still remain very abnormal and may rupture. At the very least, they would require subsequent operations and interventions.
Have there been advancements in those subsequent interventions too? What should patients who have had their aortic root replaced expect?
These subsequent interventions used to have very high mortality rates, but because of the improvements in the surgical techniques—and I’m talking about open surgical techniques in this case—these operations are done relatively safely with very good outcomes. That’s why real expertise and our true multidisciplinary approach is so important. We are literally on the cutting edge.
Awesome. Let’s move to bicuspid aortic valve disease. Any changes to treatment?
That's a very good question. The aortic valve has a very strong influence on the behavior of the proximal part of the aorta: the aortic root, ascending aorta, and the aortic arch. Bicuspid aortic valve disease is a congenital anomaly of the valve where it has only two leaflets instead of three, and it happens in about one or two percent of the population. That’s a lot of people.
And these patients usually develop aortic disease quite early in their life compared to those with normal anatomy. Approximately half require surgical repair of the aortic valve at some point.
Is that because of the location of the bicuspid valve?
That’s often what’s said. Since the aortic valve is in the proximal part of the aorta, it shares similar embryological origin, and a lot of people believe that's part of the reason why these patients have a high prevalence of aortic aneurysm.
Also, in the past five, six years or so, there are more discoveries of the hemodynamic abnormal feature of the bicuspid valve. So, when the bicuspid valve opens in a different way, it creates dilated flow within the aorta. A simple explanation of comparison would be, with a normal tri-leaflet valve, blood flows straight and then goes along the longitudinal axis of the aorta as it should. But with a bicuspid valve, the blood is ejected out from the heart hitting a particular part of the aorta. Eventually, that particular part of the aorta gets stressed and becomes dilated.
Does the advancement in imaging help here too? In understanding the hemodynamics?
Oh absolutely, yes. MRI gives us a beautiful bloodstream picture and you totally understand how the blood flows and to what direction. There is actually a spiral flow, and the images show all of that. It is fascinating. And again, with these patients, we’re talking about young and healthy people. Often they’re in their 20s and 30s.
It seems that aortic patients generally are in that younger, otherwise healthy category. Is that really the case?
It’s interesting you say that because it is definitely true, and it's becoming more and more true. It's not because the disease entity is changing but because aortic valve disease in the general sense presents in the form of aortic stenosis, a narrowing of the valve. And aortic stenosis, generally speaking, is a disease of old folks. 10 years ago, we used to do a lot of aortic valve replacements for old patients. A good 20, 25 percent of the entire practice was aortic valve replacement, but now with TAVR [Transcatheter Aortic Valve Replacement], those old folks are being treated endovascularly with a catheter.
So even with these young cohorts of patients, it’s not that the numerator has changed, it’s the denominator that’s changed. From our perspective, there is now more emphasis on these patients or a shift of care.
That’s fascinating. What’s new in research?
Starting with the context of the bicuspid aortic valve and aortic aneurysm— so even with MRI, even with the high-end echocardiogram that we discussed, both having seen enormous progress in the past several years—the normal aortic valve with three leaflets is just something that you cannot really see well. We can’t get the same level of information that we can when imaging the bicuspid valve.
With echocardiogram, you can see the structure and the function of the aortic valve, but not hemodynamics and the fluid dynamics of the aortic valve and the aortic aneurysm. And we want to see that in the aortic valve, right? In other words, we want to know how the flow is deviated, what kind of shear stress is placed where, and we just cannot do that yet with the current technology. But our group developed a way to see it!
We're using what’s called intra echocardiogram, which we often do minimally invasively through a small incision. So, what we do is examine the aortic valve by directly applying a neck probe from the small incision in the chest. And if you do that, you can visualize the aortic valve in a very, very clear way. The axis is just right to do a fluid dynamic measurement of the aortic valve.
We recently published the first and only way to visualize the fluid dynamics of the aortic valve and using that metric we've been studying the fluid dynamics of the valve itself and its relationship to the aortic aneurysm. From there, the aortic aneurysm's influence on the aortic valve, et cetera. That part of the research is very unique, first of its kind in the world, and we are very proud of it!
Incredible.
We’re also doing a clinical trial for endovascular repair of aortic arch aneurysms called the RelayBranch Trial. Generally, this type of repair has to be done through open surgery. Now, we’re doing a trial for a specific device that allows us to replace two branches out of three head vessels of the arch with endovascular therapy.
This is huge for patients who are too high risk to undergo open heart surgery. The trial is ongoing, and we’re hoping that this technology will not only allow us to treat those high-risk patients but actually create a new era of treating arch aneurysm with endovascular therapy instead of, or in addition to, open surgery.
Does this mean that due to the advancement in imaging techniques and these new devices that you expect to be able to do more and more complex repairs, multi-branch repairs, endovascularly, with minimally invasive techniques?
Yep, no doubt! Technology is only making more and more rapid progress.
Is that the way you would define progress? Procedures becoming more and more minimally invasive?
Overall as a concept, yes. The more you can with endo, the less invasive the treatment is, the better the outcomes. However, there is a caveat with endovascular therapy since it doesn't remove the aneurysm and doesn't secure the graft within the aorta. In the long term, the security of the repair may not be as good as open surgery. Now, short term outcome is certainly easier for patients and that’s an ideal option if the patients are older. But some of these patients are young, and if you're applying this technology to young and healthy patients, you do have to worry about long term outcomes.
Generally speaking, how do you make those treatment determinations?
Well, this approach began in abdominal aneurysms. For an abdominal aortic aneurysm, the vast majority of patients with “good anatomy” are now treated with the endovascular approach. Long term outcomes suggest that those patients do require subsequent procedures, or in the long run may need to be converted to an open procedure. What does that mean? It means we have to always consider long term outcomes. We must be thoughtful, thorough, and forward-thinking when choosing a treatment plan.
It is one thing to be able to do a procedure technically, but it is another thing to ensure that we are contributing to the overall health of our patients. And that is more true the more north you go in the aorta. As you move north, the aorta becomes more mobile the closer it gets to the heart, whereas, the abdominal aorta barely moves. The closer you are to the heart, the more the aorta moves, so there is more force to juggle in the area where the stent graft is placed.
Does that give you less flexibility in how or where you can place the stent or measure landing zones?
Yes, exactly, because of that force. Even if we put it in a good position, over time because of the movement, it may erode the aortic wall, et cetera. There is still room for concern, and since the technology is so new we are still learning many things. Again though, long term, endovascular therapy is the way to go because it gives you the most options. You have the option for repair or open surgery in the future. If you start with open surgery, there’s only so much you can do long term.
Since we are in this transition period, we are doing a lot of hybrid approaches. A hybrid approach is when you treat part of the aneurysm with open surgery and part of the aneurysm with the endovascular approach. Combining both together, the patient gets much less invasive therapy compared to treating all of that with open surgery.
Is that where the partnership between you and Dr. Patel really makes the difference?
Oh, working together is extremely helpful in that sense. The discussion is always, how can we create a “good anatomy” with a minimally invasive open surgery for a subsequent endovascular approach? It’s about treating aortic aneurysms in the most minimally invasive way overall. We’ll decide what kind of approach to use during the planning phase, or often, we’ll scrub in together for the open heart operation to decide the type of hybrid approach. Either a total endovascular approach, total open approach, or hybrid. And more and more frequently, we've been managing these patients with the hybrid approach.
It sounds like you’re really about creating the most options possible with the best methods available in a dynamic way, which leads right into the next question. What are you most optimistic about?
We really are! Without a doubt, endovascular therapy. The introduction or integration of this developing technology. Again, the technology is improving every year. And every year, we are dynamically changing our strategy and our thought process. V [Dr. Patel] brings in the cutting edge from his perspective with vascular, and I bring in the cutting edge from my perspective with cardiac.
Our practice is quite different even compared to what it was two years ago. That dynamic situation of aortic valve therapy itself is what's exciting, and what's great for patients. If you look at the website of any aortic surgery program they all say multidisciplinary, but there are only a handful of places in the country that work in true collaboration. It’s good to see that it is slowly changing though, we're sometimes invited to other vascular or cardio surgery programs to talk about our collaboration. It’s a true success.
Let’s end on that forward-thinking note—what are your goals for the next five to 10 years?
The goal is to make aortic therapy as minimally invasive as possible without jeopardizing the outcomes of our patients. And that’s what makes us special. We are one of the few places that can provide very different care compared to other conventional programs. It’s only going to get better and better and better.